A 72-year-old man came to us breathless. Not suddenly, but over about eighteen months, his world had been shrinking. Tasks that once cost him nothing now left him gasping. Walking, stairs, the ordinary distances of a normal day had all become negotiations with his own lungs and heart. His exercise capacity had fallen so far that the life he recognised was quietly slipping out of reach.
The cause was a valve. The aortic valve is the door the heart pushes blood through with every beat, and his had stiffened and narrowed to a fraction of its proper size. The condition is called aortic stenosis, and when it becomes severe and starts producing symptoms, it is genuinely dangerous. A heart forced to pump against a near-closed door eventually pays the price.
What makes this valve problem so easy to miss, and so important to recognise, is that its early symptoms look like simply getting older.
If you or an older relative are slowing down and putting it down to age, it is worth asking whether the heart is keeping up.
The symptoms of severe aortic stenosis tend to build gradually and include:
- Breathlessness on exertion, which is usually the first and most common sign, appearing with walking, stairs or any effort
- A steady drop in stamina, where the distance or activity you can manage keeps shrinking month by month
- Tightness or pressure in the chest during effort, sometimes mistaken for ordinary angina
- Dizziness, lightheadedness or feeling faint, especially when exerting yourself
- Episodes of passing out, which is a particularly serious warning sign
- Fatigue and a general loss of energy that creeps in over many months
The danger is that this slow, gradual pattern gets quietly accepted as the cost of getting old, when in fact it points to a mechanical problem that can often be fixed.
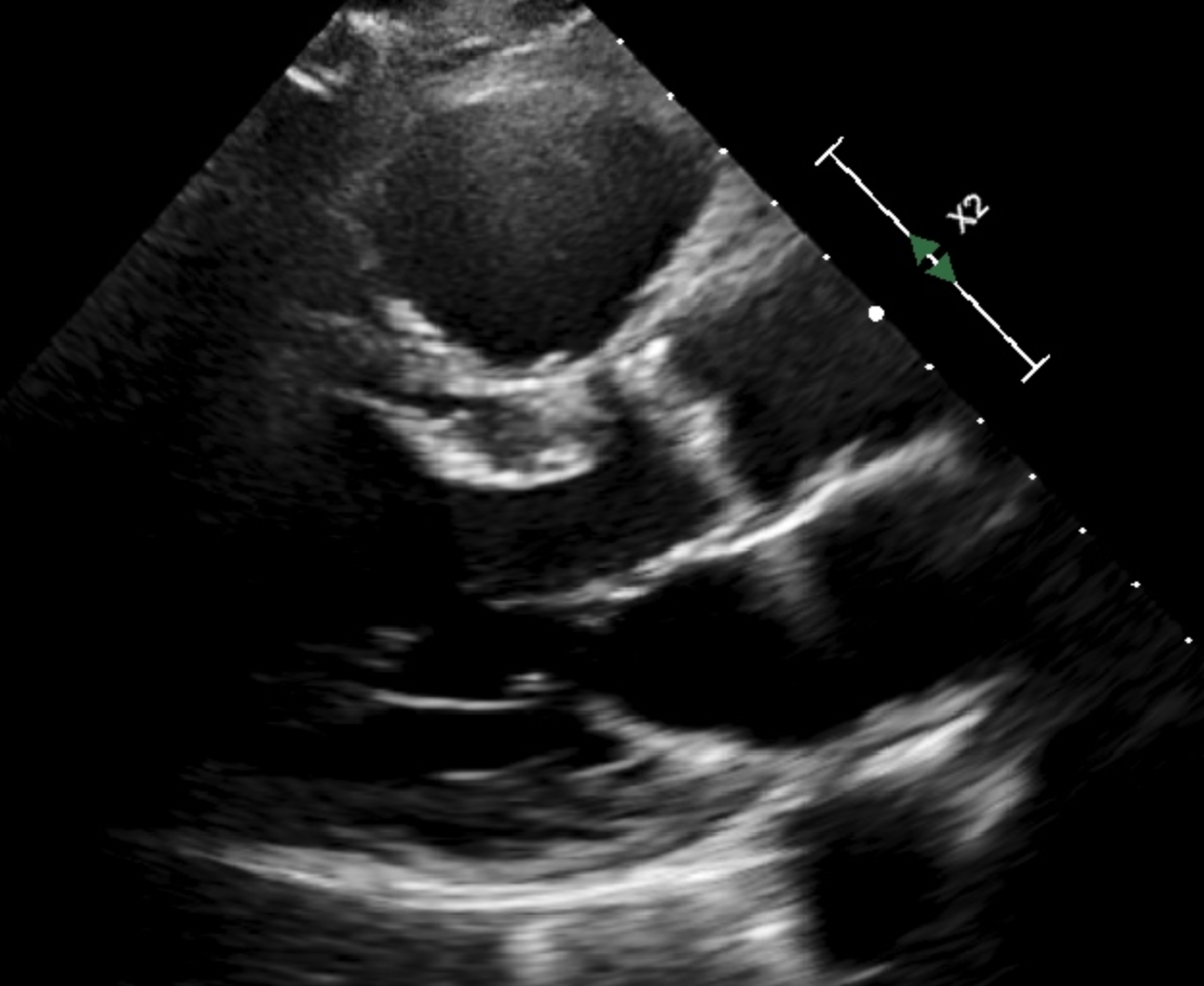
What the tests showed
His echocardiogram confirmed the worst end of the spectrum. The valve opening measured 0.7 square centimetres, against a normal area several times larger, and the pressure the heart had to generate to force blood through it was severely elevated. This was severe, symptomatic aortic stenosis, the kind that does not improve on its own and that shortens life once symptoms appear.
The complication was everything surrounding the valve. He also carried moderate COPD, he had previously suffered an ischaemic stroke, and he scored high on measures of frailty, meaning his body had less reserve to withstand a major insult. When his risk for conventional open-heart surgery was calculated formally, it came out at 8.4 percent, a figure high enough to give any surgeon real pause.
The first recommendation
The first opinion came from a regional cardiac surgery centre, and it was honest within its own walls. Open surgical replacement of the valve, known as SAVR, carries a real risk of dying on the table or never fully recovering, and for this particular man that risk was judged prohibitive. So surgery was not recommended. Instead the conversation turned to medication and palliative optimisation, which is the careful, compassionate language for managing decline rather than reversing it.
For an open-chest operation on a frail 72-year-old with lung disease and a prior stroke, calling the risk too high was not cowardice. It was an accurate assessment of that specific operation.
And there the story could easily have ended. He had been told, in effect, that his heart was too sick to fix and that the realistic plan was comfort rather than cure. Many patients in his position accept exactly this and quietly run out of time.
The second opinion
Before settling for that, he was referred to a specialised heart centre for a second opinion, and the difference was not just a different doctor. It was a different way of deciding.
Rather than one surgeon making one judgement, his case went in front of a formal multidisciplinary Heart Team, bringing several perspectives to the same table:
- Interventional cardiology, which could offer treatments that do not require opening the chest
- Cardiac surgery, to weigh the surgical options honestly alongside the alternatives
- Geriatric medicine, to assess his frailty properly and judge what he could realistically tolerate
Their conclusion was that he was not untreatable at all. He was simply unsuited to that one operation. The team chose a transfemoral TAVI, a transcatheter aortic valve implantation, in which a new valve is threaded up through an artery in the groin and seated inside the old one, with no open-chest surgery and no need to stop the heart. It is a technique developed precisely for patients whom traditional surgery would deem too high-risk.
The procedure went without complication. Six months later his symptoms had effectively vanished, classed as NYHA class I, the level reserved for people with no limitation at all. He lives independently again and goes for a walk every day.
Why this case matters
The lesson here is the hardest of the three, because the first centre was not wrong about anything it actually said.
"Too high-risk to operate" was a truthful statement about one operation at one institution. It was never a truthful statement about the patient's options as a whole.
His prognosis, it turned out, depended less on his heart than on which building he was sitting in. A centre whose main tool was open surgery reached the limit of what it could safely offer and stopped. A centre with a full Heart Team and access to transcatheter techniques saw the same frail man and saw a treatable problem. The verdict changed not because the medicine changed, but because the capabilities of the place changed.
A word of balance
None of this means the first centre failed him through negligence. It was right that open surgery was too dangerous for him, and saying so plainly was good medicine. The gap was narrower and more structural than blame allows: it could only offer what it could do, and it did not route him onward to a place that could do more.
A second opinion is especially worth seeking when:
- You or a relative are told a condition is too risky to treat, or that only palliative care remains
- The recommendation comes from a smaller or single-specialty centre rather than a multidisciplinary team
- A serious, treatable diagnosis is being managed with medication alone, without surgical or interventional options being explored
- Your instinct says there should be more on the table than you have been offered
Which leaves the question this case forces on all of us, and it is uncomfortable: when "too high-risk" is sometimes a verdict about an institution rather than a patient, whose job is it to make sure that second chance is even offered?